Diving and Ear Problems
As an avid scuba diver and a medical moderator for an online scuba forum, I answer more questions about ear problems than anything else in the context of diving. The ear is uniquely positioned to be vulnerable to both external and internal injury in this sport. Furthermore, there is a great deal of confusion about the nature of these problems - the relevant anatomy, the causes of symptoms and the best treatment.
To make things worse, even people who have obtained medical care may have no better understanding of the source of their pain, dizziness or hearing loss. This is because even for many brilliant and experienced general physicians, the ear can be difficult to examine. And while pediatricians generally have a lot of ear experience, they rarely treat scuba divers! I realize that this sounds arrogant on my part - believe me, I am humble about my own skills and deferential to GPs who must be able to manage a wide range of life threatening conditions. However, the fact remains that many doctors who are not otolaryngologists (ENTs) do not have the specialized equipment or experience necessary to clean the ear thoroughly, to examine the eardrum under high magnification, and to test hearing in a comprehensive manner.
One of the greatest sources of confusion is the fact that the outer ear, middle ear and inner ear - which are completely different systems that have very little to do with each other - often can give rise to similar symptoms such as ear pain, vertigo or hearing problems. So let's review each of the three main parts of the ear, and see how diving can affect them.
OUTER EAR
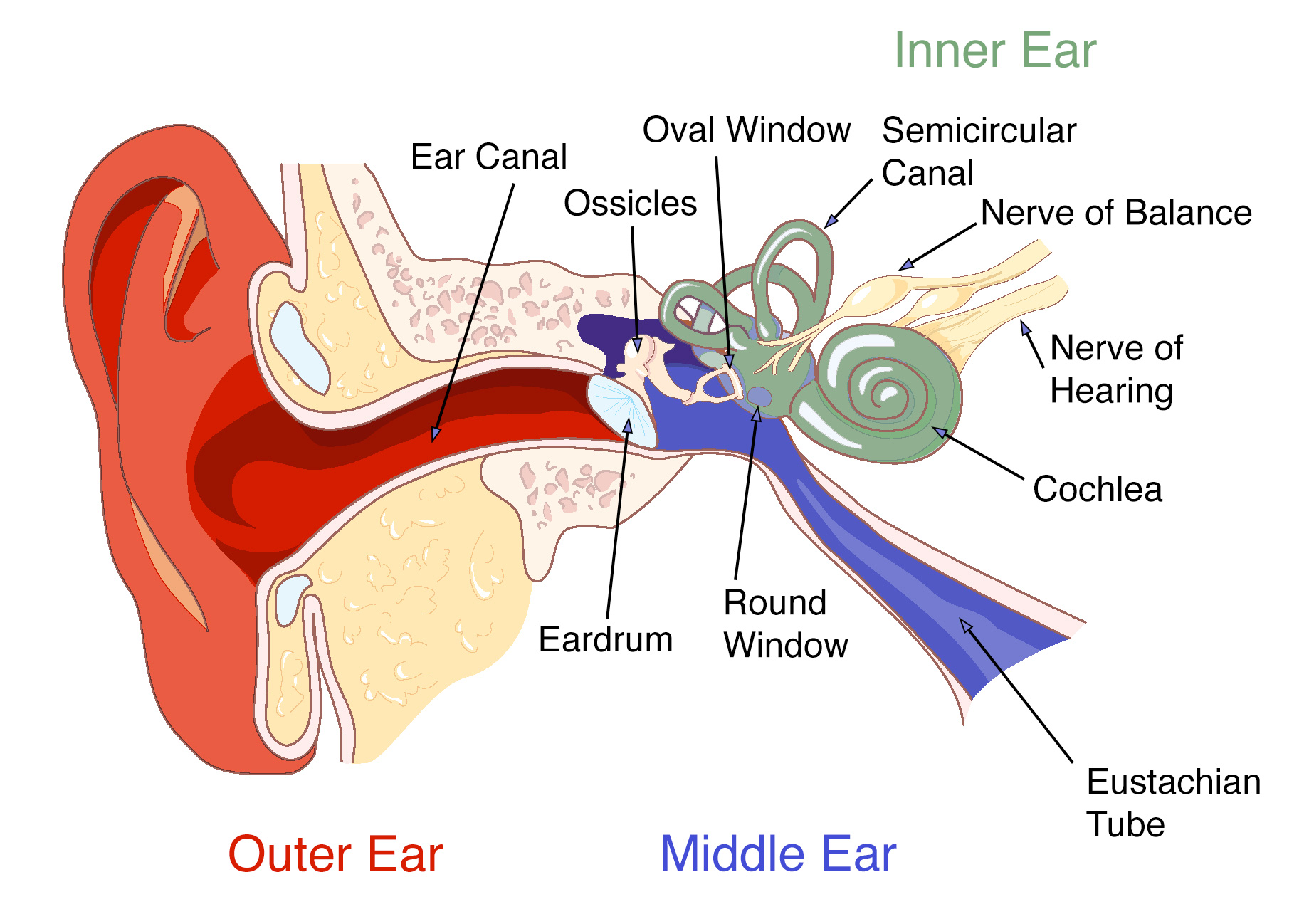
The outer ear refers to the part that sticks out of the head (the pinna) and the hole that leads to a tube (the ear canal) that ends at the eardrum. It is basically a pocket of skin, and it is where earwax (cerumen) is created and accumulates. Cerumen is a normal substance which protects the ear canal - it is generally just a thin layer coating the walls, but some people accumulate large amounts of it. It consists mostly of dead skin, mixed with various oily secretions from glands in the outer ear.
When water gets into the ear from swimming or diving, it gets into the ear canal. Unless there is a hole in the eardrum, the water from swimming or diving does not enter the middle ear.
Water from swimming or diving can get stuck in the external ear canal, especially if there is a lot of earwax. Furthermore, wet earwax takes a long time to dry out. Just like in cases of diaper rash or athlete’s foot, when an area of the body stays damp and dirty, it can lead to chronic inflammation and swelling, with skin breakdown and infection (usually with the pseudomonas bacteria that normally lives in this area). This inflammatory condition of the outer ear is called “swimmer’s ear” or otitis externa, and it can be extremely painful.
People who spend a lot of time in cold water can get bony growths in their ear canals (osteomas, or "surfer's ear"). These can trap earwax and water if they get big enough. The growths occasionally require surgical removal.
Treatment of swimmer’s ear often requires carefully cleaning the wet debris from the ear canal to allow the ear to dry. This is best done by an ENT doctor using a microscope and small ear tools, under direct vision. This will also allow for a high magnification inspection of the eardrum, to rule out a perforation or other middle ear problems. Once the ear is clean, medicated ear drops are used, generally those containing an antibiotic to kill the bacteria, and a steroid to help with the swelling and pain.
Thorough disimpaction of large accumulations of cerumen (under direct vision, ideally with a microscope) will help avoid water trapping and prevent swimmer's ear. But overly aggressive and frequent ear cleaning, especially with wax-dissolving drops, can actually make the situation worse by removing the protective layer of cerumen.
Drying the ear after swimming can help prevent this problem as well. A good way to do this is with a dedicated ear dryer, which blows a gentle stream of warm air into the ear canal. While a hair dryer can be used, an ear dryer is safer and directs the correct temperature air directly into the canal. Interchangeable tips can let family members share the device without sharing infections.
There are some ear drops that will help prevent the swelling and breakdown of the ear canal skin by lubricating the area and coating it lightly. I use something called EarShield myself when on dive trips with prolonged water exposure.
Another approach to prevention of swimmer’s ear is the use of 5-10 drops of a solution of rubbing alcohol and white vinegar after diving. Add three tablespoons of vinegar to a pint of alcohol. Unlike the 50-50 mixes which are sometimes recommended, this makes a mixture that does not have a lot of water in it. The alcohol dries the ear, and the vinegar makes the ear canal more acidic, which makes it harder for the pseudomonas bacteria to grow; you need very little vinegar for this purpose. A few drops of glycerine in the mix can help prevent overdrying. One easy way to make this is to add a small amount of white vinegar to commercially available solutions like "Swim-Ear", which is 95% isopropyl alcohol and 5% glycerine. A half of a teaspoon in the one ounce bottle is enough.
Avoid overuse of this solution, as it can overdry the ear, breaking down the protective layer of earwax and causing irritation - no more than once or twice a day. Cotton tipped applicators should never be used - they tend to pack the wax into the ear canal, and can cause permanent injury if they touch the eardrum.
MIDDLE EAR
The middle ear is the space behind the eardrum. It is lined with mucosa, which is the same sort of "skin" that lines the mouth and nose. It also contains the three bones of hearing, known as "ossicles", which carry sound vibrations from the eardrum to the inner ear (see below). The middle ear is basically an extension of the upper airway, and it is connected to the back of the nose by a tunnel called the Eustachian tube (ET). The walls of this tunnel are supported by cartilage, which tends to spring back into the normally closed position after being forced open (either by muscle action or by pressure changes in the airway from diving or from ear clearing maneuvers).
Diving injuries to the middle ear are the result of barotrauma, which is damage caused by pressure changes. As every certified diver knows, diving requires equalization of the pressure outside of the body with that inside, otherwise a big "gradient" occurs (a difference in pressure across a separating layer). This will cause pain and eventually damage. Since fluid is essentially not compressible, there are only significant pressure gradients in the air filled spaces of the body.
Most of the air in the body is in the airways - the lungs, the windpipe, the larynx (voicebox), the throat, mouth and nose. All of these spaces are connected by wide passages, so pressure changes occur everywhere at once in the airway, as a regulator delivers gas at ambient pressure (proportional to depth). It is possible to get a pressure gradient in the lungs - usually due to internal blockages of the air passages or holding the breath while ascending. While this is potentially serious, it is also quite rare.
There is also a small amount of air in other spaces in the body - the middle ear, the nasal sinuses, and sometimes the teeth (underneath dental work). These spaces are connected to the airways as well, but by small passages that may be blocked. Therefore, it is possible to build up a big pressure gradient in these spaces during descent and ascent, if a diver is not careful to equalize fully.
To equalize the ears, the diver must allow the ET to open against a pressure gradient. This can be done by a number of maneuvers taught in basic open water scuba instruction. Pinching the nose and blowing (Valsalva maneuver) and pinching and swallowing (Toynbee maneuver) are common methods for equalization, but many divers learn to open a blocked ET by other approaches, such as moving the jaw, tensing the roof of the mouth, etc...
A failure to equalize on descent can result in a block - a situation when the pressure gradient itself makes it harder for the ET to open, which results in a further gradient if descent is continued, leading to a vicious cycle and potential injury. The solution here is to stop the descent (or ascend a bit if necessary) until equalization is possible. A less common situation is a reverse block, which happens on ascent. The reason this is less common is that with a poorly functioning ET, the change in middle ear gas pressure with ascent or descent lags the change in ambient pressure. Therefore, with ascent you have higher pressure in the middle ear than in the airway. This pressure gradient tends to overcome a blocked ET - the air “forces” it’s way out. Think of how it is easier to squeeze toothpaste out of a tube than to put it back in.
A prolonged or significant pressure gradient in the middle ear can result in barotrauma. This can be a perforated eardrum (the eardrum acts like the burst disk in the scuba tank, and gives way when subjected to enough pressure). If the eardrum doesn’t perforate, fluid with or without blood can accumulate in the middle ear space. Unlike the middle ear infections that young children get, this fluid is clean with no bacteria. Clear fluid is called an “effusion”, and a bloody effusion is called a “hemotympanum”. The effusion is actually the result of fluid in the bloodstream (plasma) filtering into the middle ear when following the pressure gradient.
Fluid in the middle ear causes a temporary hearing loss by preventing the normal vibration of the eardrum with sound. It is a “conductive” hearing loss - the problem is that the mechanism that conducts sound into the inner ear is not working well. There is nothing wrong in this case with the sensory organ (the cochlea) or the nerves to the brain - if there were, it would result in a (usually permanent) “sensorineural” hearing loss, which we will discuss in the next section.
Some people have more trouble with this than others, due to dysfunction of the Eustachian tube (ETD). Many divers always need a long time to descend and ascend since their ETs don’t work very well at baseline. Other people may have no problem equalizing in general, but find it more difficult when a cold or other infection causes congestion of the lining of the ET. This is often oversimplified as the ET being "small" or "narrow" - the true problem is more of a functional issue than a structural one. Another common misconception is that fixing nasal obstruction, for example by straightening a deviated nasal septum, will help the function of the ET. While there is some overlap between nasal blockage due to an upper airway infection and ET function as mentioned above, most of the areas of the nose which require treatment to improve breathing are nowhere near the ET opening.
A single eardrum perforation related to barotrauma (without a history of ear disease) usually heals by itself over weeks to months, but no diving is allowed until the eardrum is once again intact. In some cases, surgery will be needed to seal the hole in the drum. Middle ear effusion typically resolves over time, and can be helped to resolve by the same sort of ET opening maneuvers described above. Antibiotics are generally not necessary.
Many divers swear by the use of decongestants and/or nasal steroid sprays to treat this problem or prevent its development. While these drugs can help prevent barotrauma of the nasal sinuses, there is not much data to suggest that they help middle ear disease any more than time and the ET maneuvers alone. Oral steroids can help the ears drain an effusion, but these drugs have side effects and are rarely needed in this situation. Motrin and other non-steroidal anti-inflammatory drugs may help with the pain, but have little effect on ET function. In some cases (when no more diving is planned in the near future) an ENT doctor can make a small hole in the eardrum to drain the effusion if it is causing severe symptoms (hearing loss, a blocked sensation in the ear, or dizziness).
There is not a lot that can be done directly to treat a poorly functioning ET, although there is a new procedure (balloon dilation) which may be helpful in selected cases. If the ETD is caused by a temporary problem (like a cold or other infection), then ear ventilation usually returns to baseline when the airway congestion resolves. Divers with longstanding baseline ETD usually address the problem by finding a maneuver that works to allow them to equalize.
INNER EAR
The inner ear is deep inside the skull, and is an extension of the brain. It contains the cochlea, which is the organ of hearing (like the retina in the eye) that converts sound vibrations into electrical impulses that the brain can interpret as sound. It also contains the labyrinth, which is the organ of balance. The inner ear is behind a bony wall at the back of the middle ear, and connects with the middle ear through two small holes in the bone (the round and oval windows), which are normally sealed. Unlike outer and middle ear problems, inner ear injuries cannot be seen by looking into the ear canal, although patients with inner ear barotrauma often also have middle ear injury.
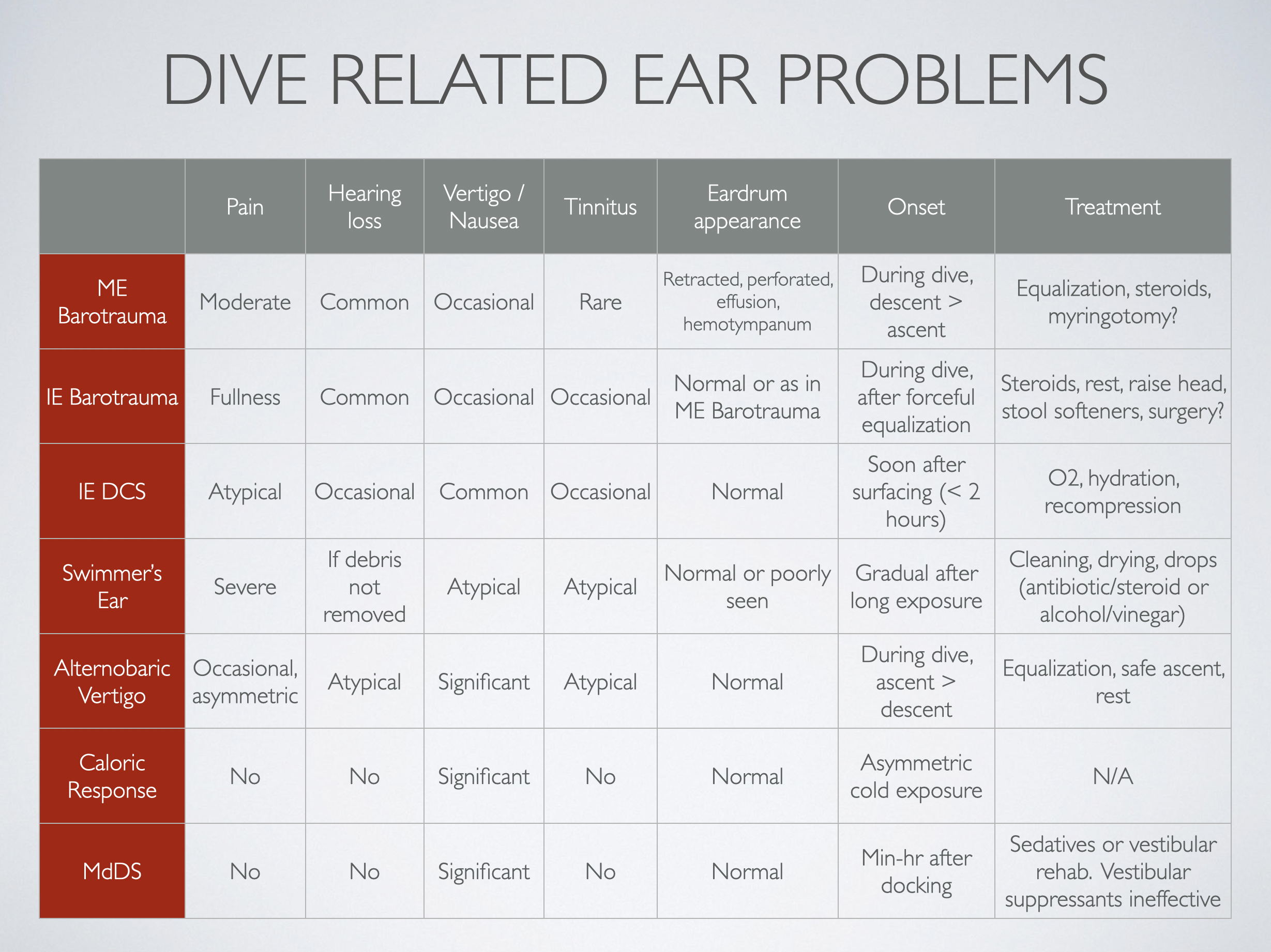
Diving related inner ear problems are very rare, but have the potential to cause permanent hearing loss. There are two main types that can result in serious injury- inner ear decompression sickness (IEDCS) and inner ear barotrauma (IEBT). These require immediate attention, and in the case of barotrauma, surgery may be necessary.
A thorough discussion of IEDCS is beyond the scope of this article, and the exact mechanism of this condition is still unclear. However, every certified diver has learned about the risk of bubble formation in the tissues with ascent, especially when inert gas (e.g. nitrogen) loading is high. IEDCS results in vertigo (and less commonly, hearing loss) when bubbles cause injury to the inner ear structures. It is not known for sure whether the injuring bubbles form in the inner ear tissue, or form elsewhere in the bloodstream and are carried to the inner ear through abnormal connections between the veins and the arteries (e.g. a patent foramen ovale or other blood vessel shunts in the lung).
IEBT can happen in a number of ways, involving a sudden pressure change in the inner ear fluid (known as perilymph). A rapid increase in middle ear pressure happens when a blocked ET suddenly opens during equalization on descent. This can cause the stapes (the bone between the middle and inner ear spaces) to be pushed sharply out of its normal position in the oval window, resulting in the inner ear fluid being pushed inward, potentially breaking the seal at the round window. A forceful Valsalva maneuver can cause an increase in inner ear pressure, pushing the round window membrane outwards, into the middle ear. Alternately, Valsalva with a blocked ET can result in pressure being transmitted the other way, as pressure in the brain rises while no corresponding rise in pressure happens in the middle ear.
This sort of trauma can result in a “perilymph fistula” (PLF) with leakage of inner ear fluid into the middle ear, potentially causing a progressive and often permanent sensorineural hearing loss, as well as vertigo and nausea. One other rare preexisting condition that can result in inner ear problems with diving is superior canal dehiscence, in which the bony covering of the inner ear is thin or missing. This can cause pressure changes to be transmitted directly to the balance organ of the inner ear.
Diagnosis of inner ear problems can be difficult, as the eardrum can normal on exam. Treatment for IEDCS and IEBT is very different, and recompression of a patient with IEBT can actually make the ear injury worse. Some authors have suggested that if the diagnosis is uncertain, holes should be made in the eardrums (myringotomy) before entering the chamber to prevent this complication. In actual practice, this is rarely necessary as the two conditions have different presenting features.
IEDCS may be suggested by the dive profile - excessive nitrogen loading, rapid or multiple ascents, aggressive decompression plans or skipped decompression stops. Also, there is usually a short symptom free interval after surfacing, with the vertigo generally starting within two hours. Symptoms of IEBT, on the other hand, usually develop during the dive, often following a forceful equalization. In both conditions, there may be nystagmus - rapid movements of the eye away from the injured inner ear.
Prior to decompression, all patients with any sort of suspected decompression illness should be treated with 100% oxygen and hydration (if conscious and able to drink). Even if the diagnosis is actually IEBT, there is no harm of doing this, so this initial treatment should not be delayed because of any uncertainty.
A formal hearing test can distinguish between conductive and sensorineural hearing loss, and therefore should be a part of the evaluation of any diving related ear injury. Other tests include an assessment of the function of the balance mechanism, which can be measured in a special lab. A CT scan is rarely helpful, as an acquired PLF caused by barotrauma cannot be seen on an x-ray.
When there is enough of a suspicion of a PLF, an operation may be recommended; this condition can only be definitively diagnosed by surgical exploration of the ear (you can't see the inner ear fluid by looking in the ear canal). The procedure involves lifting up the eardrum to visualize the middle ear directly. If what looks like inner ear fluid is seen leaking from the space around the round window (or anywhere else), fat grafts are used to seal the area. This leakage can be very subtle, as the volume of perilymph is small. However, early closure of a PLF can mean the difference between a recovery of hearing and a progression to complete deafness. Since the operation itself involves very little risk, it should be strongly considered in cases where PLF is a possibility.
Ear symptoms without the risk of permanent damage can be caused by other conditions that arise during diving. The one thing these have in common is a lack of normal inputs from the sensory organs to the brain. Either asymmetric signals from each ear, or inconsistent information from the ears and the eyes will result in nausea, vomiting or vertigo - this is the brain's response to such confusing inputs.
The balance organ of the inner ear (the semicircular canals) can be cooled by exposure to water in the ear canal, which causes the fluid inside the canals to move - this is a cold caloric response. If one ear is exposed to more cold water than the other - because of a poor fitting hood or wax in one ear canal - the brain will get different signals from each ear. Similarly, if one ear equalizes before the other, there will be a pressure difference between the ears, with differential stimulation of the inner ear sensory mechanisms. This is known as altenobaric vertigo.
Both of these conditions are generally temporary, and resolve as the temperature stabilizes and the flow stops, or as equalization is completed in both ears. However, it can be very disconcerting to have sudden dizziness during a dive. Awareness of this phenomenon and taking any steps necessary to address it (such as careful and thorough equalization) can prevent a spiral into panic and bad decisions.
Another condition well known to boat divers is sea sickness. Here, the vertigo is caused by inconsistency between the inputs to the brain from the eyes and the ears. If you are on a moving boat, your ears are telling your brain that you are moving up and down in space. But if your eyes are looking at any part of the boat, they will send the signal that you are standing still. This is why staring at the horizon helps sea sickness - it coordinates the information received by the brain from the ears and the eyes.
Finally, there is the condition known as Mal de Debarquement ("the sickness of getting off a boat"). Some people are unsteady and have difficulty walking after reaching dry land. This is thought to be an issue with the brain's adaptation to a new environment, and not an ear problem. In such cases, inner ear testing is normal, but the symptoms may last for a long time (months). Treatment with vestibular suppressants (like Bonine or Dramamine) rarely works, but sedatives and specialized physical therapy (vestibular rehabilitation) may be helpful.
CONCLUSION
The vast majority of ear pain after diving goes away by itself in a short time. However, without an examination, a diver may not be able to tell whether the problem is in the outer or middle ear, and treatment depends on accurate diagnosis. Hearing loss after diving should be evaluated soon, ideally with formal hearing testing. Thorough evaluation of persistent ear problems should be done by a doctor with the tools and experience necessary to distinguish outer, middle and inner ear disease.

As an avid scuba diver and a medical moderator for an online scuba forum, I answer more questions about ear problems than anything else in the context of diving. The ear is uniquely positioned to be vulnerable to both external and internal injury in this sport. Furthermore, there is a great deal of confusion about the nature of these problems - the relevant anatomy, the causes of symptoms and the best treatment.
To make things worse, even people who have obtained medical care may have no better understanding of the source of their pain, dizziness or hearing loss. This is because even for many brilliant and experienced general physicians, the ear can be difficult to examine. And while pediatricians generally have a lot of ear experience, they rarely treat scuba divers! I realize that this sounds arrogant on my part - believe me, I am humble about my own skills and deferential to GPs who must be able to manage a wide range of life threatening conditions. However, the fact remains that many doctors who are not otolaryngologists (ENTs) do not have the specialized equipment or experience necessary to clean the ear thoroughly, to examine the eardrum under high magnification, and to test hearing in a comprehensive manner.
One of the greatest sources of confusion is the fact that the outer ear, middle ear and inner ear - which are completely different systems that have very little to do with each other - often can give rise to similar symptoms such as ear pain, vertigo or hearing problems. So let's review each of the three main parts of the ear, and see how diving can affect them.
OUTER EAR
The outer ear refers to the part that sticks out of the head (the pinna) and the hole that leads to a tube (the ear canal) that ends at the eardrum. It is basically a pocket of skin, and it is where earwax (cerumen) is created and accumulates. Cerumen is a normal substance which protects the ear canal - it is generally just a thin layer coating the walls, but some people accumulate large amounts of it. It consists mostly of dead skin, mixed with various oily secretions from glands in the outer ear.
When water gets into the ear from swimming or diving, it gets into the ear canal. Unless there is a hole in the eardrum, the water from swimming or diving does not enter the middle ear.
Water from swimming or diving can get stuck in the external ear canal, especially if there is a lot of earwax. Furthermore, wet earwax takes a long time to dry out. Just like in cases of diaper rash or athlete’s foot, when an area of the body stays damp and dirty, it can lead to chronic inflammation and swelling, with skin breakdown and infection (usually with the pseudomonas bacteria that normally lives in this area). This inflammatory condition of the outer ear is called “swimmer’s ear” or otitis externa, and it can be extremely painful.
People who spend a lot of time in cold water can get bony growths in their ear canals (osteomas, or "surfer's ear"). These can trap earwax and water if they get big enough. The growths occasionally require surgical removal.
Treatment of swimmer’s ear often requires carefully cleaning the wet debris from the ear canal to allow the ear to dry. This is best done by an ENT doctor using a microscope and small ear tools, under direct vision. This will also allow for a high magnification inspection of the eardrum, to rule out a perforation or other middle ear problems. Once the ear is clean, medicated ear drops are used, generally those containing an antibiotic to kill the bacteria, and a steroid to help with the swelling and pain.
Thorough disimpaction of large accumulations of cerumen (under direct vision, ideally with a microscope) will help avoid water trapping and prevent swimmer's ear. But overly aggressive and frequent ear cleaning, especially with wax-dissolving drops, can actually make the situation worse by removing the protective layer of cerumen.
Drying the ear after swimming can help prevent this problem as well. A good way to do this is with a dedicated ear dryer, which blows a gentle stream of warm air into the ear canal. While a hair dryer can be used, an ear dryer is safer and directs the correct temperature air directly into the canal. Interchangeable tips can let family members share the device without sharing infections.
There are some ear drops that will help prevent the swelling and breakdown of the ear canal skin by lubricating the area and coating it lightly. I use something called EarShield myself when on dive trips with prolonged water exposure.
Another approach to prevention of swimmer’s ear is the use of 5-10 drops of a solution of rubbing alcohol and white vinegar after diving. Add three tablespoons of vinegar to a pint of alcohol. Unlike the 50-50 mixes which are sometimes recommended, this makes a mixture that does not have a lot of water in it. The alcohol dries the ear, and the vinegar makes the ear canal more acidic, which makes it harder for the pseudomonas bacteria to grow; you need very little vinegar for this purpose. A few drops of glycerine in the mix can help prevent overdrying. One easy way to make this is to add a small amount of white vinegar to commercially available solutions like "Swim-Ear", which is 95% isopropyl alcohol and 5% glycerine. A half of a teaspoon in the one ounce bottle is enough.
Avoid overuse of this solution, as it can overdry the ear, breaking down the protective layer of earwax and causing irritation - no more than once or twice a day. Cotton tipped applicators should never be used - they tend to pack the wax into the ear canal, and can cause permanent injury if they touch the eardrum.
MIDDLE EAR
The middle ear is the space behind the eardrum. It is lined with mucosa, which is the same sort of "skin" that lines the mouth and nose. It also contains the three bones of hearing, known as "ossicles", which carry sound vibrations from the eardrum to the inner ear (see below). The middle ear is basically an extension of the upper airway, and it is connected to the back of the nose by a tunnel called the Eustachian tube (ET). The walls of this tunnel are supported by cartilage, which tends to spring back into the normally closed position after being forced open (either by muscle action or by pressure changes in the airway from diving or from ear clearing maneuvers).
Diving injuries to the middle ear are the result of barotrauma, which is damage caused by pressure changes. As every certified diver knows, diving requires equalization of the pressure outside of the body with that inside, otherwise a big "gradient" occurs (a difference in pressure across a separating layer). This will cause pain and eventually damage. Since fluid is essentially not compressible, there are only significant pressure gradients in the air filled spaces of the body.
Most of the air in the body is in the airways - the lungs, the windpipe, the larynx (voicebox), the throat, mouth and nose. All of these spaces are connected by wide passages, so pressure changes occur everywhere at once in the airway, as a regulator delivers gas at ambient pressure (proportional to depth). It is possible to get a pressure gradient in the lungs - usually due to internal blockages of the air passages or holding the breath while ascending. While this is potentially serious, it is also quite rare.
There is also a small amount of air in other spaces in the body - the middle ear, the nasal sinuses, and sometimes the teeth (underneath dental work). These spaces are connected to the airways as well, but by small passages that may be blocked. Therefore, it is possible to build up a big pressure gradient in these spaces during descent and ascent, if a diver is not careful to equalize fully.
To equalize the ears, the diver must allow the ET to open against a pressure gradient. This can be done by a number of maneuvers taught in basic open water scuba instruction. Pinching the nose and blowing (Valsalva maneuver) and pinching and swallowing (Toynbee maneuver) are common methods for equalization, but many divers learn to open a blocked ET by other approaches, such as moving the jaw, tensing the roof of the mouth, etc...
A failure to equalize on descent can result in a block - a situation when the pressure gradient itself makes it harder for the ET to open, which results in a further gradient if descent is continued, leading to a vicious cycle and potential injury. The solution here is to stop the descent (or ascend a bit if necessary) until equalization is possible. A less common situation is a reverse block, which happens on ascent. The reason this is less common is that with a poorly functioning ET, the change in middle ear gas pressure with ascent or descent lags the change in ambient pressure. Therefore, with ascent you have higher pressure in the middle ear than in the airway. This pressure gradient tends to overcome a blocked ET - the air “forces” it’s way out. Think of how it is easier to squeeze toothpaste out of a tube than to put it back in.
A prolonged or significant pressure gradient in the middle ear can result in barotrauma. This can be a perforated eardrum (the eardrum acts like the burst disk in the scuba tank, and gives way when subjected to enough pressure). If the eardrum doesn’t perforate, fluid with or without blood can accumulate in the middle ear space. Unlike the middle ear infections that young children get, this fluid is clean with no bacteria. Clear fluid is called an “effusion”, and a bloody effusion is called a “hemotympanum”. The effusion is actually the result of fluid in the bloodstream (plasma) filtering into the middle ear when following the pressure gradient.
Fluid in the middle ear causes a temporary hearing loss by preventing the normal vibration of the eardrum with sound. It is a “conductive” hearing loss - the problem is that the mechanism that conducts sound into the inner ear is not working well. There is nothing wrong in this case with the sensory organ (the cochlea) or the nerves to the brain - if there were, it would result in a (usually permanent) “sensorineural” hearing loss, which we will discuss in the next section.
Some people have more trouble with this than others, due to dysfunction of the Eustachian tube (ETD). Many divers always need a long time to descend and ascend since their ETs don’t work very well at baseline. Other people may have no problem equalizing in general, but find it more difficult when a cold or other infection causes congestion of the lining of the ET. This is often oversimplified as the ET being "small" or "narrow" - the true problem is more of a functional issue than a structural one. Another common misconception is that fixing nasal obstruction, for example by straightening a deviated nasal septum, will help the function of the ET. While there is some overlap between nasal blockage due to an upper airway infection and ET function as mentioned above, most of the areas of the nose which require treatment to improve breathing are nowhere near the ET opening.
A single eardrum perforation related to barotrauma (without a history of ear disease) usually heals by itself over weeks to months, but no diving is allowed until the eardrum is once again intact. In some cases, surgery will be needed to seal the hole in the drum. Middle ear effusion typically resolves over time, and can be helped to resolve by the same sort of ET opening maneuvers described above. Antibiotics are generally not necessary.
Many divers swear by the use of decongestants and/or nasal steroid sprays to treat this problem or prevent its development. While these drugs can help prevent barotrauma of the nasal sinuses, there is not much data to suggest that they help middle ear disease any more than time and the ET maneuvers alone. Oral steroids can help the ears drain an effusion, but these drugs have side effects and are rarely needed in this situation. Motrin and other non-steroidal anti-inflammatory drugs may help with the pain, but have little effect on ET function. In some cases (when no more diving is planned in the near future) an ENT doctor can make a small hole in the eardrum to drain the effusion if it is causing severe symptoms (hearing loss, a blocked sensation in the ear, or dizziness).
There is not a lot that can be done directly to treat a poorly functioning ET, although there is a new procedure (balloon dilation) which may be helpful in selected cases. If the ETD is caused by a temporary problem (like a cold or other infection), then ear ventilation usually returns to baseline when the airway congestion resolves. Divers with longstanding baseline ETD usually address the problem by finding a maneuver that works to allow them to equalize.
INNER EAR
The inner ear is deep inside the skull, and is an extension of the brain. It contains the cochlea, which is the organ of hearing (like the retina in the eye) that converts sound vibrations into electrical impulses that the brain can interpret as sound. It also contains the labyrinth, which is the organ of balance. The inner ear is behind a bony wall at the back of the middle ear, and connects with the middle ear through two small holes in the bone (the round and oval windows), which are normally sealed. Unlike outer and middle ear problems, inner ear injuries cannot be seen by looking into the ear canal, although patients with inner ear barotrauma often also have middle ear injury.
Diving related inner ear problems are very rare, but have the potential to cause permanent hearing loss. There are two main types that can result in serious injury- inner ear decompression sickness (IEDCS) and inner ear barotrauma (IEBT). These require immediate attention, and in the case of barotrauma, surgery may be necessary.
A thorough discussion of IEDCS is beyond the scope of this article, and the exact mechanism of this condition is still unclear. However, every certified diver has learned about the risk of bubble formation in the tissues with ascent, especially when inert gas (e.g. nitrogen) loading is high. IEDCS results in vertigo (and less commonly, hearing loss) when bubbles cause injury to the inner ear structures. It is not known for sure whether the injuring bubbles form in the inner ear tissue, or form elsewhere in the bloodstream and are carried to the inner ear through abnormal connections between the veins and the arteries (e.g. a patent foramen ovale or other blood vessel shunts in the lung).
IEBT can happen in a number of ways, involving a sudden pressure change in the inner ear fluid (known as perilymph). A rapid increase in middle ear pressure happens when a blocked ET suddenly opens during equalization on descent. This can cause the stapes (the bone between the middle and inner ear spaces) to be pushed sharply out of its normal position in the oval window, resulting in the inner ear fluid being pushed inward, potentially breaking the seal at the round window. A forceful Valsalva maneuver can cause an increase in inner ear pressure, pushing the round window membrane outwards, into the middle ear. Alternately, Valsalva with a blocked ET can result in pressure being transmitted the other way, as pressure in the brain rises while no corresponding rise in pressure happens in the middle ear.
This sort of trauma can result in a “perilymph fistula” (PLF) with leakage of inner ear fluid into the middle ear, potentially causing a progressive and often permanent sensorineural hearing loss, as well as vertigo and nausea. One other rare preexisting condition that can result in inner ear problems with diving is superior canal dehiscence, in which the bony covering of the inner ear is thin or missing. This can cause pressure changes to be transmitted directly to the balance organ of the inner ear.
Diagnosis of inner ear problems can be difficult, as the eardrum can normal on exam. Treatment for IEDCS and IEBT is very different, and recompression of a patient with IEBT can actually make the ear injury worse. Some authors have suggested that if the diagnosis is uncertain, holes should be made in the eardrums (myringotomy) before entering the chamber to prevent this complication. In actual practice, this is rarely necessary as the two conditions have different presenting features.
IEDCS may be suggested by the dive profile - excessive nitrogen loading, rapid or multiple ascents, aggressive decompression plans or skipped decompression stops. Also, there is usually a short symptom free interval after surfacing, with the vertigo generally starting within two hours. Symptoms of IEBT, on the other hand, usually develop during the dive, often following a forceful equalization. In both conditions, there may be nystagmus - rapid movements of the eye away from the injured inner ear.
Prior to decompression, all patients with any sort of suspected decompression illness should be treated with 100% oxygen and hydration (if conscious and able to drink). Even if the diagnosis is actually IEBT, there is no harm of doing this, so this initial treatment should not be delayed because of any uncertainty.
A formal hearing test can distinguish between conductive and sensorineural hearing loss, and therefore should be a part of the evaluation of any diving related ear injury. Other tests include an assessment of the function of the balance mechanism, which can be measured in a special lab. A CT scan is rarely helpful, as an acquired PLF caused by barotrauma cannot be seen on an x-ray.
When there is enough of a suspicion of a PLF, an operation may be recommended; this condition can only be definitively diagnosed by surgical exploration of the ear (you can't see the inner ear fluid by looking in the ear canal). The procedure involves lifting up the eardrum to visualize the middle ear directly. If what looks like inner ear fluid is seen leaking from the space around the round window (or anywhere else), fat grafts are used to seal the area. This leakage can be very subtle, as the volume of perilymph is small. However, early closure of a PLF can mean the difference between a recovery of hearing and a progression to complete deafness. Since the operation itself involves very little risk, it should be strongly considered in cases where PLF is a possibility.
Ear symptoms without the risk of permanent damage can be caused by other conditions that arise during diving. The one thing these have in common is a lack of normal inputs from the sensory organs to the brain. Either asymmetric signals from each ear, or inconsistent information from the ears and the eyes will result in nausea, vomiting or vertigo - this is the brain's response to such confusing inputs.
The balance organ of the inner ear (the semicircular canals) can be cooled by exposure to water in the ear canal, which causes the fluid inside the canals to move - this is a cold caloric response. If one ear is exposed to more cold water than the other - because of a poor fitting hood or wax in one ear canal - the brain will get different signals from each ear. Similarly, if one ear equalizes before the other, there will be a pressure difference between the ears, with differential stimulation of the inner ear sensory mechanisms. This is known as altenobaric vertigo.
Both of these conditions are generally temporary, and resolve as the temperature stabilizes and the flow stops, or as equalization is completed in both ears. However, it can be very disconcerting to have sudden dizziness during a dive. Awareness of this phenomenon and taking any steps necessary to address it (such as careful and thorough equalization) can prevent a spiral into panic and bad decisions.
Another condition well known to boat divers is sea sickness. Here, the vertigo is caused by inconsistency between the inputs to the brain from the eyes and the ears. If you are on a moving boat, your ears are telling your brain that you are moving up and down in space. But if your eyes are looking at any part of the boat, they will send the signal that you are standing still. This is why staring at the horizon helps sea sickness - it coordinates the information received by the brain from the ears and the eyes.
Finally, there is the condition known as Mal de Debarquement ("the sickness of getting off a boat"). Some people are unsteady and have difficulty walking after reaching dry land. This is thought to be an issue with the brain's adaptation to a new environment, and not an ear problem. In such cases, inner ear testing is normal, but the symptoms may last for a long time (months). Treatment with vestibular suppressants (like Bonine or Dramamine) rarely works, but sedatives and specialized physical therapy (vestibular rehabilitation) may be helpful.
CONCLUSION
The vast majority of ear pain after diving goes away by itself in a short time. However, without an examination, a diver may not be able to tell whether the problem is in the outer or middle ear, and treatment depends on accurate diagnosis. Hearing loss after diving should be evaluated soon, ideally with formal hearing testing. Thorough evaluation of persistent ear problems should be done by a doctor with the tools and experience necessary to distinguish outer, middle and inner ear disease.